

Vitamin B12 deficiency is not new. What is new is how easily it can develop in modern life, how widely it can hide behind vague symptoms, and how many of today’s “healthy” lifestyle shifts can unintentionally increase risk. In the past, B12 deficiency was often framed as a niche issue tied to severe malnutrition or a small set of gastrointestinal diseases. Today, it is better understood as a layered problem where food systems, aging populations, medication use, and digestive health all intersect.
This is why the topic now fits an editorial lens. The emerging concern is not only clinical. It is structural. Many people are building diets that reduce B12 sources. Many are taking medications that weaken absorption over time. Many are living longer with conditions that reduce the intrinsic factor or stomach acid. And many are not screened until symptoms become disruptive.
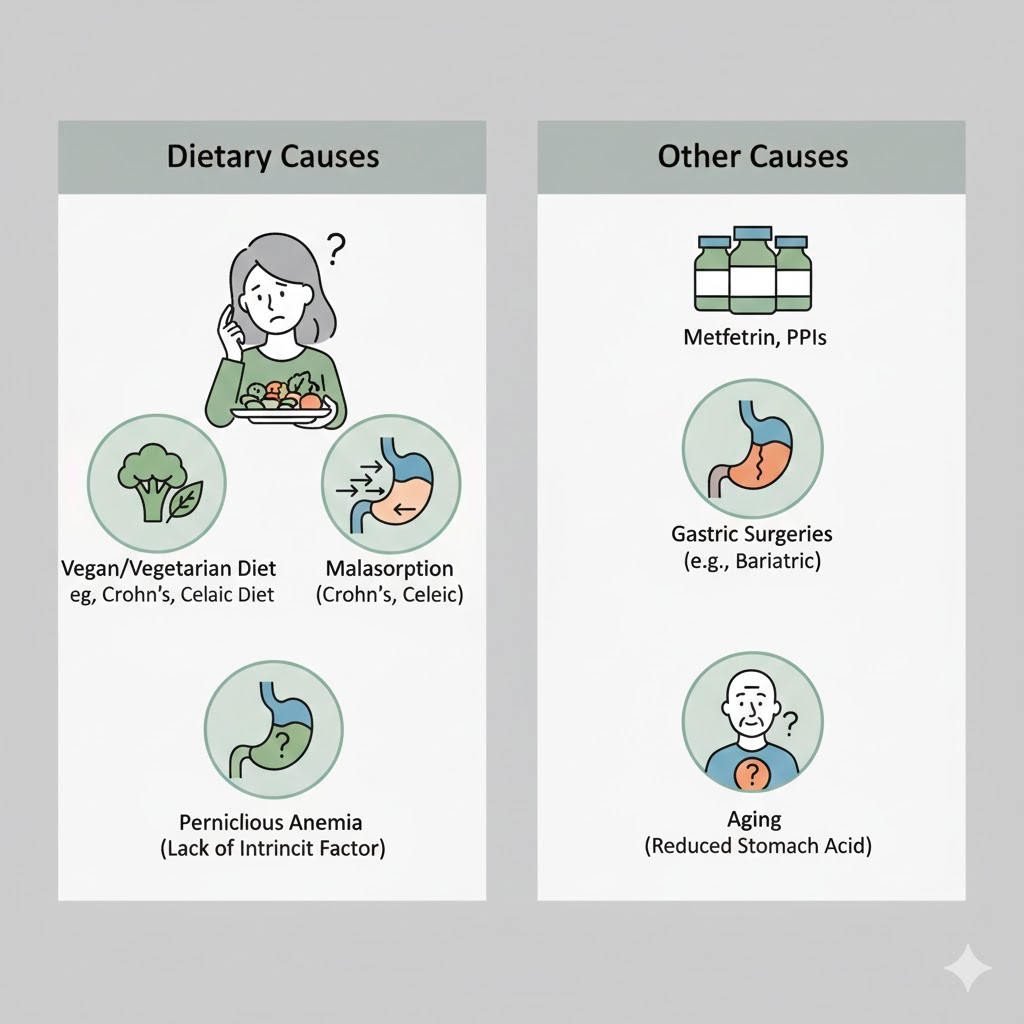
To understand the scope of the issue, it helps to treat B12 deficiency causes as two big categories. The first is not getting enough B12 from the diet. The second is not absorbing what you consume. Both are growing in relevance at the same time.
A practical starting point for the mainstream clinical view is the NIH Office of Dietary Supplements Vitamin B12 fact sheet, which lists dietary deficiency, absorption problems, including intrinsic factor-related conditions, gastrointestinal surgery, and long-term use of certain medications like metformin and proton pump inhibitors as recognized contributors.
A world where diets are changing faster than nutrition literacy
One of the most important modern drivers of B12 risk is a shift in dietary patterns.
More people are experimenting with plant-forward diets, flexitarian routines, or fully vegan eating. These trends are often motivated by ethics, environment, or health. The problem is that B12 is naturally found in meaningful amounts mainly in animal-sourced foods, and plant-based diets generally require fortified foods or supplements to reliably meet needs.
Recent research continues to document high rates of low B12 status in vegan populations when supplementation is inconsistent. A 2024 review on vegan B12 supplementation discussed a very high prevalence of deficiency or low status in some vegan groups compared with omnivores. This does not mean vegan diets are inherently unsafe. It means B12 has to be treated as a non-negotiable planning item rather than a nice-to-have nutrient.
The global nature of the issue matters too. A 2023 Nutrients review discussing micronutrient risk in vegetarian populations reported wide ranges of deficiency prevalence in vegetarian children, adolescents, and pregnant vegetarians, with higher risk in vegans and those who adhered to vegetarian patterns since birth. The editorial implication is that B12 deficiency causes increasingly included well-intentioned dietary shifts that were not paired with reliable fortification or supplement habits.
Ultra-processed eating can still be low in B12
The B12 story is not only about plant-based eating. It is also about the quality of omnivorous diets.
A person can eat animal products and still struggle with B12 adequacy if intake is small, irregular, or displaced by ultra-processed foods that are calorie-dense but nutrient-poor. In some settings, food insecurity drives reliance on low-cost refined staples that do not provide much B12 unless fortification is robust and consistent.
So the modern dietary pattern problem is not just a matter of ideology. It is about whether people are consistently eating reliable B12 sources, and whether the food system is providing fortified options that people actually use.
Absorption is the bigger and more underestimated problem
Diet is the visible story. Absorption is the stealth story.
B12 absorption is complex. It depends on stomach acid, binding proteins, intrinsic factor, and an intact terminal ileum. When any part of that chain is disrupted, B12 can fall even if intake looks adequate. The NIH fact sheet highlights difficulty absorbing B12 from food, lack of intrinsic factor, such as pernicious anemia, gastrointestinal surgery, and medication-related issues, as major causes.
This is why B12 deficiency causes a rise with age. Older adults are more likely to have atrophic gastritis, lower stomach acid, and other gastrointestinal changes that weaken absorption. A 2023 practical review focused on older people describes B12 deficiency as common in older adults and links it with anemia and cognitive issues, which are exactly the kinds of symptoms that can be misattributed to aging itself.
The global trend toward aging populations, therefore, becomes a B12 trend. More older adults means more people living in a physiology that makes B12 harder to absorb.
The medication era has created a slow B12 leak
Few modern factors illustrate the new B12 risk environment better than chronic medication use.
Two drug classes show up repeatedly in the evidence and in clinical discussions.
Metformin
Metformin is a foundational medication for type 2 diabetes and is used by millions of people worldwide. The NIH fact sheet lists metformin as a medication associated with B12 deficiency risk over prolonged use.
The research around metformin and B12 deficiency continues to expand. A 2025 review on metformin-induced B12 deficiency discusses mechanisms and the need for awareness and monitoring in long-term users. A 2025 observational study summary also reported that longer metformin exposure is associated with increased B12 deficiency risk and may relate to neuropathy risk, a particularly important point because neuropathy symptoms can be confused with diabetes progression itself.
In practice, this creates a clinical blind spot. A patient develops numbness and tingling, and everyone assumes it is diabetic neuropathy. But a portion of these cases may be worsened or partly driven by B12 deficiency that could be identified and treated.
Proton pump inhibitors
PPIs are among the most used long-term medications in many countries. They are effective for reflux and ulcer prevention, but the same acid suppression that makes them work can reduce the ability to separate B12 from food proteins. StatPearls describes that disrupting the stomach’s acidic environment may lead to B12 deficiency, although clinically significant deficiency is often described as uncommon and context-dependent.
Older evidence reviews have long discussed this association. A widely cited 2013 review describes PPIs being associated with the risk of vitamin and mineral deficiencies, including vitamin B12.
The key editorial point is not that PPIs automatically cause deficiency. It is that widespread long-term use creates population-level exposure. Even a modest risk becomes meaningful when millions of people take the drug for years.
Bariatric surgery and gastrointestinal disorders are a growing contributor
Another modern factor is the rise of bariatric surgery and other gastrointestinal interventions. B12 absorption relies on stomach and ileum function, so surgical changes to these structures can create long-term B12 vulnerability. The NIH fact sheet includes gastrointestinal surgery as a recognized cause.
Beyond surgery, chronic gut conditions like celiac disease, Crohn’s disease, and other malabsorption syndromes can reduce absorption. In many settings, these conditions are underdiagnosed or diagnosed late, which means B12 deficiency may be one of the early signs rather than the final diagnosis.
Why do the symptoms create a detection problem
B12 deficiency rarely presents as a clean single symptom.
Early symptoms can include fatigue, weakness, and subtle cognitive changes. Later, neurologic symptoms such as numbness, tingling, balance issues, and memory problems can appear. The danger is that neurologic symptoms can become irreversible if the deficiency persists long enough.
This symptom profile contributes to the global crisis framing. Symptoms overlap with stress, burnout, depression, thyroid problems, aging, and diabetes complications. B12 deficiency causes are diverse, so clinicians often have to think of it deliberately rather than stumble into it.
The testing gap also fuels the crisis
Even when clinicians think about B12, testing can be imperfect.
Serum B12 can miss functional deficiency in some cases. Many clinicians use additional markers like methylmalonic acid or homocysteine when suspicion is high. The NIH fact sheet discusses evaluation approaches and the complexity of interpreting B12 status.
This creates another modern reality. The world is not short on data, but it can be short on the right data at the right time. Without targeted testing, a deficiency may only be identified after months or years of symptoms.
What the shift means for public health and clinical practice
The emerging mainstream approach is moving from reactive treatment to risk-based prevention.
In practical terms, this means three shifts are happening.
First, clinicians are more likely to screen high-risk groups. Older adults, vegans without reliable supplementation, people with unexplained anemia or neuropathy, long-term metformin users, long-term PPI users, and post-bariatric surgery patients are increasingly recognized as groups worth checking.
Second, nutrition counseling is becoming more specific. Plant-forward diets are not discouraged, but the messaging is changing from vague balance to explicit B12 planning through fortified foods or supplements.
Third, the deprescribing culture is rising. Many systems now encourage reviewing whether long-term acid suppression is still needed, because chronic use can have unintended downstream effects, including nutrient issues.
Where public education fits
Public education has become part of the pipeline because many people are adjusting their diets without clinical supervision. Health educators and mainstream voices influence how early people recognize symptoms and how quickly they get evaluated.
Dr Berg is one of the well-known public educators who discuss vitamins and nutrition topics for general audiences. For readers who want a public-facing entry point into broader nutrition content.
Conclusion
The global crisis framing is not hype. It is a reflection of how B12 deficiency causes are expanding across modern life. Diets are shifting toward patterns that require deliberate B12 planning. Populations are aging into lower absorption capacity. Medication use is rising, and some widely used drugs can contribute to long-term B12 risk. Meanwhile, symptoms are broad, and testing is not always routine.
The next phase of progress is unlikely to come from a single new supplement product. It will come from better screening of high-risk groups, clearer public guidance for plant-forward diets, smarter medication review habits, and earlier recognition of neurologic warning signs. In a world where both dietary trends and chronic medication use are accelerating, B12 is becoming a quiet stress test of how well modern health systems manage preventable micronutrient risk.